As we approach the July 1st Canada Day weekend we remember to celebrate the blessings and bounties our Nation has given us. For me its the new life I was given by a lung transplant eleven years ago, thanks to my donor and Dr. Shaf Keshavjee, at Toronto General Hospital. This recent article in The Toronto Star highlights his achievements.
Toronto lung transplant surgeon leading innovations to boost donor organ pool
“I think the impact of this will be changing the 15 per cent world utilization (for donated lungs) to 50 per cent. That is more than tripling the number of lung transplants done around the world,” Keshavjee says. “This came from here and it’s going to impact the world.”
The Toronto Star
Toronto surgeon Dr. Shaf Keshavjee’s innovations are transforming how lung transplants are done. He has lead the development of the Toronto XVIVO Perfusion System, which treats and improves high-risk donor lungs so they can be safely used for transplant.

Dr. Shaf Keshavjee, seen in the hall of Toronto General Hospital immediately after he performed a double-lung transplant in February, has received the Order of Ontario for his innovative work in his field.
Dr. Shaf Keshavjee apologizes as his BlackBerry keeps buzzing. He is receiving emails from the Trillium Gift of Life Network, Ontario’s organ and tissue donation agency.
They are offering him a pair of lungs — organs from an individual whose identity must be kept secret for ethical reasons, and likely the victim of a recent accident, head injury or brain hemorrhage — from some undisclosed location in Canada.
Keshavjee, director of the Lung Transplant Program at Toronto General Hospital, part of the University Health Network, peers closely at the screen of the mobile device. He is looking at an x-ray of the organs. The image is tiny, but to his trained eye, he can tell the organs are less than perfect.
“There is some abnormality because there is some lightness to it,” he says, pointing to a couple of minuscule white dots.
The lungs are the most fragile of all the organs and injuries to this pair may have been sustained during whatever tragedy led to the donor’s brain death. Or after, when resuscitation attempts were made. Or even after that, when the body was kept alive on life support.
Typically, such damaged lungs would not be considered for transplant. Indeed, an average of only 15 per cent of donated lungs end up being used worldwide.
But because of innovations led by Keshavjee, Toronto General is now able to use 40 per cent of the lungs offered. And Keshavjee is working to raise that number.
For his efforts, he was recently recognized with the Order of Ontario and two Queen’s Jubilee medals. His accomplishments are indeed an Ontario success story. His innovations are transforming lung transplant surgery around the world.
Keshavjee types a response on his BlackBerry, telling Trillium he will take the lungs.
“Smartphones have made it a lot easier. I can do this lying in my bed in the middle of the night. And I do,” he says.
So begins the complex process that will ultimately lead to someone who is dying of lung disease getting a transplant.
There are more than 80 Ontarians waiting for either a lung or a heart-lung transplant. About 20 per cent of them will die on the waiting list.
For Keshavjee, who has done about 400 lung transplants, this is just another day at the office.
“I will have a recipient ready tonight at midnight to start fitting the lungs in,” says the 51-year-old transplant surgeon who is now planning to work into the next day.
This is only one of Keshavjee’s jobs. He is also surgeon-in-chief at the University Health Network, a researcher, medical school professor and thoracic surgeon who does elective surgery, mostly on lung cancer patients.
His biggest claim to fame is leading the development of the Toronto XVIVO Perfusion System (ex vivo means outside the body), which treats and improves high-risk donor lungs so they can be safely used for transplant.
A couple of weeks after the initial interview, Keshavjee allows a reporter and photographer to tag along to see how the system works.
A pair of lungs arrives at the hospital in a blue Coleman cooler at 10:30 a.m. on a Monday. They were harvested from an anonymous donor’s body, somewhere in Canada, six hours earlier.
While a family somewhere in Canada grieves for the loss of the donor, a man in his 60s with advanced chronic obstructive pulmonary disease is being prepped for transplant surgery. He’s excited and jittery, too nervous to be interviewed by a reporter.
Besides, it’s difficult to talk. He needs 100 per cent oxygen at all times just to stay alive.
At this point, it’s not certain whether the transplant will even go ahead. The donor lungs are in bad shape, inflamed and full of fluid.
The lungs arrive in operating room 18, the organ regeneration laboratory, on the second floor of the hospital. A team of about six medical professionals is already assembled. They include surgeons, nurses and perfusion specialists who operate the XVIVO system.
There are also research fellows from Hong Kong, Chile, Spain and Brazil. Professionals from every major transplant center around the world have come through the hospital to learn the technique.
The lungs are removed from the cooler and placed into a bucket of ice. A tube is attached to the pulmonary artery, which normally delivers blood to the lung from the heart. Another tube is sewn to a vein that normally drains blood out of the lung.
The organs are then moved to a steel table in the center of the room atop of which sits the XVIVO device. Also known as “the bubble,” it resembles a glass-domed cake plate.
Here, the lungs are hooked up to a circuit that includes a ventilator and heart-lung machine, which pumps a preservation solution into them. The solution, made of low-potassium dextran, was initially developed by Keshavjee and later perfected by others.
As the lungs are brought back up to body temperature, they are healed with a type of anti-inflammatory therapy, also developed by Keshavjee, which makes them less prone to malfunction.
Like something out of a science fiction novel, the lungs eventually begin inflating and deflating. The disembodied organs are alive, breathing on their own.
“It’s something I wouldn’t have imagined seeing in my lifetime,” says Keshavjee, who still marvels at the accomplishment.
Keshavjee bustles around the hospital while the lungs recover on the XVIVO system. He has a couple of meetings, a clinic with cancer patients and an interview with a candidate for a nurse navigator position.
He continuously checks on the lungs, calling the OR, visiting in person and even checking in via Skype on an iPad.
The XVIVO team updates him with results of ongoing tests. They assess the lungs’ function with blood gases, x-rays and bronchoscopies. They check the resistance to the flow of fluid through the lungs and whether the organs are becoming less stiff.
They also pump them with anti-inflammatory drugs and antibiotics.
The lungs continue to improve and at the four-hour mark, Keshavjee makes the call. The surgery can go ahead.
Another benefit of the XVIVO system is that it allows doctors to know how lungs will function before they are transplanted, thereby reducing the risk of death.
“I already know that the lungs are going to work before I even start the operation. That is transformative. Before, you would find out after,” Keshavjee says.
He continues with his other duties around the hospital, while another operating room is made ready for the transplant surgery and the patient is told the good news.
Seven hours after the lungs arrived at the hospital, the transplant begins.
The room is filled with music from Keshavjee’s iPod: Hedley, Florence and the Machine, Lady Gaga. His 15-year-old daughter’s selection.
In Keshavjee’s tool kit are more than 100 sterilized surgical instruments, including different sizes of clamps, forceps, scissors and what look like wrenches. There are even power tools.
Keshavjee opens the patient’s chest horizontally using an electric sternum saw so that it lifts like the hood of a car.
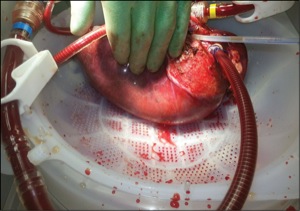
He removes and replaces the lungs one at a time. When the first one comes out, the signs of disease are apparent. It is bright red with inflammation and black lines run through it.
It takes the surgeon only 45 minutes to sew in each new lung. He expertly sutures them to the patient’s bronchus, pulmonary artery and veins, attaching them to the heart.
Each lung is slowly re-perfused with the patient’s own blood. Within minutes, the thousands of tiny blood vessels in the organs fill.
The right lung is done first. It inflates as it fills for the first time with the transplant patient’s own breath of air.
“When you stop to think about what we are doing, it is pretty amazing,” Keshavjee exclaims.
Before the patient is sewn up, samples of his new lungs are taken for research.
Keshavjee has big plans to take the technology even further by modifying transplanted lungs with gene therapy and stem cell therapy so they that patients don’t need to take anti-rejection drugs. Ultimately, he hopes to be able to build new lungs.
“Can you strip all the cells out of it, keep the skeleton, the scaffold and then take your bone marrow, your stems cells and build a lung that is you?”
Twelve hours after the surgery, the patient is removed from the ventilator. Where he had difficulty breathing with oxygen support before, he is now easily breathing on his own.
The day after the surgery, he is out of his bed and able to eat a meal of clear fluids.
One of the first things that strikes the patient is that he can get through a meal without have to stop for a break to catch his breath.
“It’s just a simple thing, but he can’t recall when he was last able to do that,” Keshavjee says.
Without the transplant and the ability to salvage lungs that were otherwise unusable, there was a more than 50 per cent chance the man would have died within the year.
The Toronto XVIVO Perfusion System has saved this man and has the potential to save many more lives as other countries adopt it. There are plans to use it for other organs, aside from lungs, as well.
“I think the impact of this will be changing the 15 per cent world utilization (for donated lungs) to 50 per cent. That is more than tripling the number of lung transplants done around the world,” Keshavjee says.
“This came from here and it’s going to impact the world.”
In Ontario, you can register your consent to be an organ and tissue donor online at beadonor.ca.
“You Have the Power to Donate Life – Sign-up today! Tell Your Loved Ones of Your Decision”